 Methylation is a biochemical process that involves the addition of a methyl group to a molecule (CH3). In the context of genetics and molecular biology, methylation commonly refers to the addition of a methyl group to DNA or RNA molecules. Methylation can affect gene expression and it plays a role in about 200 various biological processes.
Methylenetetrahydrofolate reductase (MTHFR) is an important enzyme involved in the methylation cycle; it can limit the methylation that can happen in the body. The MTHFR gene dictates the process for making the enzyme MTHFR. MTHFR is critical for a chemical reaction involving vitamin folate (B9). It enables the conversion of a form of folate called, 5,10-methylenetetrahydrofolate to a different form of folate called methyltetrrahydrofolate (5-MTHFR). This is the main kind of folate found in the bloodstream and is a primary component of the composite process that converts the amino acid homocysteine to another amino acid called methionine. The body uses methionine to make proteins and other important compounds. The primary role of methylation is to recycle the amino acid homocysteine to keep its levels in a healthy, optimal range. A simple homocysteine blood test can help you understand your own methylation status. High homocysteine levels indicate suboptimal methylation and need attention to decrease the level and to help bring your levels to a healthy range. Nutrition plays a big role in how smoothly methylation processes run. Taking targeted supplements can support healthy methylation as well as eating foods rich in folate, vitamin B12, vitamin B6, riboflavin, choline, and Coenzyme Q10. As part of the initial workup with me, you can expect a lab for the MTHFR gene, homocysteine, folate, B12, and many others. Note, if you do have a mutation in the MTHFR gene, it is essential to follow guidelines on treatment throughout your life. It is not something you do for a while and stop. Here are some symptoms to watch for if you suspect you may struggle with poor methylation (but of course, get the lab done!): Nervous system issues, gut dysbiosis, thyroid dysfunction, insomnia (especially REM phase), anxiety, depression, heart problems and addiction. While science is still understanding methylation and other detoxification pathways, it is well understood that poor methylation is beneficial with folate. Should you not know your status on the MTHFR, this would be worthy to have blood drawn.
0 Comments
“Sometimes you hear a voice through the door calling you, as fish out of water hear the waves, or a hunting falcon hears the drum’s come back. This turning toward what you deeply love saves you.” - RUMI This blog is the continuation on the topic of the Four Balances taken from my five-week retreat on Cultivating Emotional Balance Teacher’s Training (CEBTT). The focus of this blog will investigate Conative Intelligence. Conative intelligence is an aspect of our mental life that compels us into a certain direction for what we desire or want to achieve. In contemplating the first of the Four Balances within CEBT, we may relate to the meaning of Conative Intelligence as the quality of intention, aspiration, will, volition, motivation. All of which under penetrating insight reveals itself as a deep yearning for flourishing. If we attune our lives purposefully for what we desire and commit to it’s unfolding, while appearing at first blush as a simple task, it becomes an exercise of dedication and courage.
Our modern lives have taken the shape of long work days; kids in childcare; fast food restaurants; Starbuck’s to keep us going; 100+emails each day; multiple texts messages; phone calls; managing finances; cleaning the house; maybe some exercise; going to movies; concerts and other entertainments; sex ... oh did someone mention time for that; and sleeping maybe six hours, etc. You get the picture. Where is the time to even consider what you truly aspire for in life, when what’s being dished up is modernity in full throttle? In assessing Conative Intelligence, one aspect of conation is the knowledge that we make choices in how we spend our time. The act of free will often has turned into the perception of “I have to, because … fill in the blank.” Another aspect to Conative Intelligence is to strive for something or the ambition to achieve something. Again this striving and ambition has become a plethora of demands yanking at us for attention. Yet, inquiring more deeply into the nature of Conative Intelligence, qualities of serenity, stillness, compassion, kindness, and wisdom are revealed. So how in the world has such intelligence been hijacked by modernity that promised us peace, love, and light? We made choices with our free will in our striving and ambitions and placed our source of happiness on people, places, and things. The old cliché’ of “looking for love in all the wrong places.” Thankfully, at any moment, we can choose otherwise with our free will and place our efforts and attention on our heart’s desire and to know our Conative Intelligence. So let’s begin with turning our attention toward this innate goodness that has all the fossil fuel, so to speak, to guide us toward our hearts true desire. This is not a promise of drinking the Kool-Aid, because attending to our hearts true desire does take courage, dedication, perseverance, kindness, and a re-arrangement of our current circumstances (to some degree, at least). Everyday, begin the day with this simple mindfulness practice. As we investigate our lives in this daily practice, note insights that arise, emotions that surface, and sensations that arise and where they are located. Begin this practice with finding a comfortable position and take notice of your breath and allow your body to relax and be at ease. Focus on your in-and-out breath for a few moments. Now begin your vision quest journey. Ask yourself the following four questions. This is not an exercise in finding a “right” answer, but instead to allow the question to sit within you and answer itself. This is not an exercise in mental projections, but rather an exercise of inquiry into the hearts perceptive. Now ask yourself these questions (it helps to record these and listen while in meditation):
(Source: Visions Quest questions from Alan B. Wallace, PhD) In the words of Christopher Reeves, a true Superman with an indelible spirit, said, “So many of our dreams at first seem impossible. Then they seem improbable, and then, when we summon the WILL, they soon became inevitable.” May your true hearts desire flourish and be brought alive, because for each of us, the world needs it now.  If you are experiencing weight gain, it is time to have your insulin levels measured.
Insulin is a peptide hormone made in the pancreas when levels of glucose are detected in the gut that are elevated. Glucose is a simple sugar and a primary source of energy for the body’s cells. Glucose enters the body in forms of monosaccharides (fruit sugar), disaccharides (milk sugar) or polysaccharides (starch). When in excess, the cells store as glycogen which is used in states of fasting or energy necessity. The hormone insulin coordinates with glucagon to modulate glucose levels. Insulin acts via an anabolic pathway, while glucagon performs catabolic functions. Insulin binds to cell receptors, acting as a gatekeeper, shuttling glucose into cells to be processed into energy, or ATP (adenosine triphosphate). Or it induces glucose storage in the liver, muscles, and adipose tissue, which when in excess will cause weight gain. Insulin can be added to a lab draw which is essential in understanding metabolic status. While the range on a standard lab test is about 2-24 mIU/ml, an optimal range is between 2-6. Because insulin is the fat storage hormone, as the level increases above 6, more fat storage will take place. As weight begins to increase, mainly around the waistline, insulin resistance ensues causing metabolic dysfunction. This increases the risk of chronic diseases such as diabetes, heart disease, cancer, and dementia. Within the cell are mitochondria (please listen to the short audio on mitochondria) and these ancient bacteria are responsible for glucose conversion into ATP. However, as insulin rises, the waist increases and toxic levels of glucose circulate in the bloodstream, the mitochondria are damaged. Less energy is produced in the cell due to this damage and a typical symptom reported by patients is low energy. There is good news. Reducing the burden on the mitochondria due to excess carbohydrate intake and reducing stress levels (which do cause the breakdown of glucose storage from the liver and muscles) will over time decrease insulin levels (less fat storage). Monitoring insulin levels, A1c, and glucose are standard labs drawn within my practice. If you are gaining weight or have excess weight, it is time to get those levels measured. From there, a treatment plan, which may include medications, is prescribed and I will help get you on your way to an optimal weight and lifestyle plan.  We’ve all had those nights where we toss and turn and sleep seems far off. Many of us grab for melatonin supplements in hopes of warding off the dark nights of insomnia. Studies are not conclusive as to whether it helps sleep and whether long-term use is safe. What is melatonin? How does it work?
Melatonin is a hormone, a potent anti-inflammatory, an antioxidant which is used for other purposes than sleep. Because of its properties, melatonin is being used in cancer therapies, autoimmunity, post-COVID syndrome, Polycystic Ovary Syndrome (PCOS), infertility, bone health, gut health, and other disease states. Melatonin is released by the pineal gland in response to darkness. It regulates the circadian rhythm and circulates throughout the body and acts upon the “clock genes.” The liver and kidneys rapidly metabolize melatonin within an hour when taken as a synthetic supplement so only fractions of it will stay in the bloodstream while sleeping. It is suggested in some studies to help with primary sleep disorders, decrease sleep latency and improve sleep quality compared to placebo. Yet it is important to remember that our endogenous melatonin being secreted by the pineal gland provides a steady state while sleeping (only with darkness) and slowly decreases within the last several hours prior to waking. The mitochondria (small structures in a cell that are found in the cytoplasm — the fluid that surrounds the cell nucleus) regulate most of our melatonin most likely in relation to oxidative processes via an enzyme defense. The body’s way to protect itself and scavenge free radicals. However, there is a threshold of protection the mitochondria can withstand and not become overloaded. Melatonin declines with age sometime after puberty and precipitously after around age 50. Supplementation of only 0.3mg would be needed to replace levels; however, that amount may not cover a person’s need and you would need to assess each person, individually. Foods rich in melatonin include tart cherries, coffee, beetroot, asparagus, sprouted kidney beans, extra virgin olive oil, St. John’s war, feverfew, to name a few. These foods have a rich source of phytomelatonin; however, in very minute amounts. Before rushing out to start melatonin, always think lifestyle first. To help induce natural production, darkness is necessary. Staying away from blue light, light within the environment, keeping a dark bedroom, or consider wearing an eye mask, are the first lines intervention. Of course, exercise, stress, fasting/eating, room temperature, sleep apnea, etc., are also significant to helping with sleep beyond what melatonin can do. Take home advice: love to like the darkness in your environment and begin tapering the lights about 2 hours before bedtime. May you find darkness as a soothing and relaxing friend that will welcome melatonin. One of my favorite tests in assessing hormone status, is the DUTCH (Dried Urine Test for Comprehensive Hormones) test used for comprehensive hormone testing. Production of our hormones occurs from an elaborate process via cholesterol and enzyme conversions. Ultimately, hormones are detoxified and then need to be excreted via stool, urine and sweat. This pathway is vital in hormonal health. Let’s break this pathway down. See figure 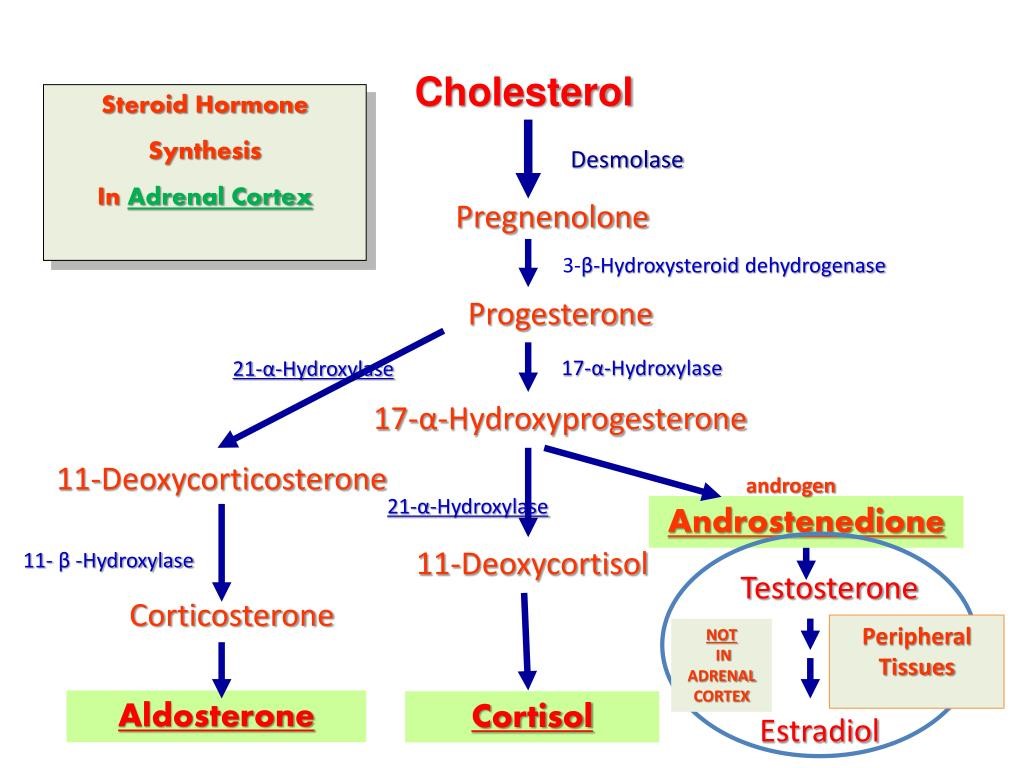 Cholesterol can get a bad rap without deserving it, but thanks to “Big Pharma,” it has been vilified specifically the LDL-c (low dense lipoprotein-cholesterol). Hormone replacement therapy has been looped into the “bad” category as well and is also misunderstood. Let’s take a look at how cholesterol (LDL-c) converts to hormones. Within the liver, cholesterol will begin its part of the metabolism process to become hormones via enzymes breaking it from one hormone into another one. Enzymes are necessary as well as co-factors to start the process of this steroid-hormone pathway. It is a downstream process. As the diagram reflects, cholesterol’s first hormone conversion is pregnenolone (a hormone naturally produced in the body by the adrenal gland). On one side of that conversion, progesterone is made. Progesterone (a hormone released by the corpus luteum in the ovary) has enzymes that cleaves (adheres to or sticks to) it into metabolites which can then be detoxified and will then enter the bowels, bladder and sweat glands for excretion. The same process occurs for our androgens, testosterone, cortisol, and estrogens, and also neurotransmitters, caffeine, alcohol, etc. The DUTCH test will reflect how your body does this breakdown. When you lack an enzyme and/or cofactors (i.e., folate, B12, zinc, etc.), the hormone pathway can be shunted in another direction and create a burden elsewhere. And remember, there are many endocrine disruptors in our environment that enter these pathways to be metabolized and compete at hormone receptor sites and/or create a huge toxic burden within this pathway. Ultimately, these hormones become metabolites. Also, 2-hydroxy (2-OH-E1) is considered the protective pathway, while 4-OH-E1 and 16-OH-E1 are oxidative in nature and cause DNA damage. Think of the rusting process that could occur on a car-that’s oxidation. When I review your DUTCH test, we will make a treatment plan on how to help your detoxification pathway to better excrete toxic metabolites. Remember that your bowel habits, water intake and exercise inducing sweating, help these toxins leave the body and why they are pivotal to hormone health. When prescribing bio-identical hormone therapy (BHT), it is essential to have this testing done on a regular basis along with other laboratory testing.  Hormonal declines are inevitable and when it arrives at our doors, the symptoms can be mild to a staggering feeling of exhaustion, depression, and not belonging to one’s own skin any longer. Symptoms include weight gain, mood changes, hot flashes, insomnia, joint pain, no sex drive, brain fog, and low energy. The neurohormonal shifts begin a decline in bone loss (osteopenia/osteoporosis), cholesterol changes atherosclerosis (hardening of the arteries caused by buildup of plaque), cognitive decline (Alzheimer’s), collagen loss (skin elasticity, wrinkles), vaginal atrophy (painful sex), and cortisol/stress hormone fluctuations (weight gain especially around the waist).
Bioidentical Hormone Replacement Therapy (BHRT), which is FDA-approved (except when compounded — a custom formulation of medication to fit a unique need of a patient), has been shown in research to reduce rates of heart disease, osteoporosis, Alzheimer’s, and vaginal atrophy. On the other hand, risks may include blood clots, stroke, and Myocardial Infarction (heart attack). However, because there is no long-term data with bioidentical hormones, the risks are not known. The studies for these side effects come from Premarin® and Provera® (conjugated estrogens) which are not bioidentical and taken in oral form. When I prescribe BHRT, I have them compounded and have them in patch, trouche (lozenges that dissolve slowing in the mouth), suppository or liquid form; they do not pass through the liver on its first phase of metabolism and where oral estrogen pass through the liver which is the reason the rate of blood clots increases. The oral birth control pill has the same risk due to the first pass in the liver. When patients initially establish care with me, labs and DUTCH test are necessary to assess their baseline hormonal status. The timing for starting BHRT is paramount to make sure bone density is established as well as warding off other disease processes. Once BHRT are prescribed, I require a yearly DUTCH test and labs. To remain as an established patient, the minimum visits will be two times per year. Most patients on average see me three times per year. Appointments can be conveniently held via telemedicine. "It takes no time to fall in love, but it takes years to know what love is." - Singer-songwriter Jason Mraz Romance is a hot topic and the romance novel industry knows something about as it brings in a whopping 1 billion annually. We are interested in keeping romance alive, yet while time passes most relationship will be plagued with the romance blues. Researcher, Helen Fisher, details her findings in the Chemistry of Love. Fisher’s research explores the various neuro-hormonal pathways of love, the longevity of such chemicals, and theorizes the idea of a love map.
Many factors are contributory toward the decline and the rate at which couples may experience the diminishing romantic feelings, such as each partner’s sexual constitution, lifestyle, health, finances, work schedule, children, living situation, religion, etc. Also, one’s expression of romance is important to understand to ensure that their love language is conveyed in a way that is received. Bottom line is we are wired to connect. Within a very complex neural network, we have a reward motivational system that is activated when we encounter a potential mate. This juices up the system with dopamine and norepinephrine. This system gives us the craving for that person leading to focused attention, obsessive thinking, and euphoria. We may relate to this as “the fall.” Serotonin which helps regulate moods, emotions, sleep and appetite drops during this phase, which causes the lack of appetite, reduced sleep and emotions and moods that feel uncontrollable. Our bonding hormone, Oxytocin ensures the attachment and provides the peace and calm we feel when in their presence. Of course, testosterone needs mentioning as this propels us into the pursuit and desire for sex. Once sexual activity takes place, these hormones and neurotransmitters go into overdrive to essentially ensure procreation and pair bonding. However, there is the caveat. It’s a short-lived experience. It’s essentially not sustainable. The question becomes how to create sustainability and satisfaction for both partners. First and foremost, hormones levels are important to know as hormone replacement may be all it takes to ignite the desire and pursuit of romance. Of course, communicating wants and needs is fundamental to a healthy bonded relationship. Stella Resnick, PhD., a leading researcher in keeping the spark alive in long-term relationships, says there are three distinct behaviors these couples exhibit with each other. First, they eye gaze and attune to their partner. Secondly, they touch each other and hold hands often. Lastly, they have continued kissing one another throughout their relationship. As a sexuality counselor, these behavior are usually absent from couples I see. Training in these behaviors alone, gives the kick start. From there, scheduling dates, doing activities together that arouse a sense of excitement and fun together, and mostly, it’s the true desire to want to engage with each other with an authentic and connecting approach. Cheers! Over the past 25 years, Neuroscience is exponentially growing elucidating the positive influence meditation has on our health. Cultivating constructive qualities of mind such as lovingkindness, compassion, gratitude, and empathy, continue to provide very rich data of the neuro-hormonal activations that occur essentially priming our systems with good health. Multiple brain regions are involved in the generating the embodied process of these mental states. Studies are often cross-linking, reporting many of the same brain area activations that stimulate the nervous system, giving us the elixir of well-being.
Last year, the University of Southern California’s Brain and Creativity Research Institute released a research paper, Neural Correlates of Gratitude. Eminent Neuroscientist Dr. Antonio Demasio was one of the researchers, which brought my attention to this article. The study hypothesized that brain regions associated with moral cognition, value judgment, and theory of mind would be activated. These areas are seen to be activated in the above mentioned mind states as well. In eliciting the quality of gratitude, various scenarios drawn from the Holocaust were told to the participants. Stories ranged from being given food, a place to sleep, and someone saving their life. Participates were asked to put themselves into that experience (which is an empathic experience) and rate their level of gratitude, 1-rating lower level of gratitude and 4-rating high. There were 26 participants, none of which had any connection to the Holocaust. The overall rating was 2.6. The participants stated they felt as if they could live in the experience that the Holocaust survivor had lived and the gratitude that must have been felt. As researchers hypothesized, the area of the Prefrontal Cortex, the seat of moral cognition, was activated, as well as, regions associated with prosocial behavior, interpersonal relationships, and social support. Gratitude considered a virtue in all religions, does appear to have a place in the brain. With the stimulus of imagining a scenario to elicit gratitude, we can activate the center of moral cognition affiliated with positive emotion and mental well-being. While many of us know the felt sense of practicing gratitude, this study, demonstrates the neurological correlates. Also remembering, our brains are neuroplastic, therefore, what we fixate on wires neurons, for better or worse. We are wired to experience gratitude as this study suggests. Our brain circuitry has gifted us with a byproduct of gratitude when we have benefited from the goodwill of another, imagined or real. Not only that, but he next byproduct of this experience is resiliency, emotional stability, and well-being. Amazing, how we are gifted again. With gratitude and may all being know gratitude. " She’s crazy. Just when you think you’ve reached the bottom of her craziness, there’s a crazy underground garage." - Anonymous Many of us have had that brush with the type of boyfriend or husband that is like riding Full Throttle at Magic Mountain. Even you guys out there know what I’m talking about. I’m sure you’ve been dazzled in the elixir of the love-hate relationship just the same. These theme park-like relationships seem to be very common experiences in partnering. Even the fad diets and exercise programs offer this yo-yo style relationship with ourselves, yet 95% of the time, they fail to yield any lasting happiness.
In my health and sexuality practices, I’ve contemplated the dilemma of how the relationships with our bodies, genitalia, love relationships, exercise, food, etc. … resembles the love-hate dramas of relationships that exist. No offense guys, but I call these relationships “the bad-boyfriend syndrome.” While we know that half of marriages end in divorce, how many relationships have you encountered the wild ride of the love-hate game. Now here's some data about how we have a love-hate relationship with ourselves. Research suggests that 91% of women dislike their bodies. And currently, about 8 million people suffer from eating disorders, while the weight loss industry revenue tops $55 billion dollars annually. It gets better. The cosmetic industry revenue is $58 billion annually and the fashion industry, sit down for this one, is 1.2 trillion dollars annually. Somehow we spend a lot of money attempting to “love” ourselves/bodies, yet most women are still very unsatisfied with them, seems like some internal aggression toward ourselves. This roller coaster of fabricating a sense of love toward ourselves with a new outfit, more Botox, another boyfriend/girlfriend, a new diet plan, a new pair of underwear to entice but don’t get to cozy down there because you don’t like the way it looks, smells, taste, is the cycle of this syndrome. In John Mayer’s song, The Heart of Life, he sing’s “fear is a friend who is misunderstood.” As I coach clients about this dualistic framework on the love-hate dynamic at play, fear shows itself with a mighty presence. Fear reveals the secret to healing. It’s certainly a very edgy, scary, and less traveled involvement we have with this emotion, and, unfortunately, the data tells the story. Americans are billions and trillions of dollars away from their fears. The thing with our fear though, is we can’t break up with it and leave it at another house. It’s a shadow that follows us so closely and intimately. The mega bucks spent on avoidance will never produce the most reliable love of our life called facing our fears. The capitalistic monkey at play in this story is not interested in our befriending this energy, in fact, it would become crippled if we did actually engage with it in a meaningful and loving way. We each want that relationship with a partner that is loving, kind, compassionate, thoughtful, and delicious, but you know the story of this. We must first have it within to have it on the outside. There are transformative exercises and methods to transform these fearful emotions into a warm regard and love for ourselves. We can make friends with our fears. We can stop searching for something that a mega-wealthy industry distracts us from and begin to love ourselves anew. As Rumi says, "maybe you are searching among the branches, for what only appears in the roots." For coaching on your fears, contact Sherri through her website. “The true function of sex is to bring more love into the world.”
- Diana Richardson As I reflect upon the years as a Sex Counselor and consider the root of the problems couples have with their sexuality, it seems to boil down to passionless sex. While that seems like an obvious statement, I’d like to share the depth of what I mean by that statement. While there are many causes and conditions that merge together creating sexual dissatisfaction from couple to couple, what I have witnessed over the years may be distilled down to that simple statement, passion burnout. We can turn to the current state of affairs in the typical American bedroom. The average time a couple spends on foreplay is 10-19 minutes and intercourse is about 7 minutes. Yet for woman, igniting the female arousal system takes about 40 minutes to fully engage. While some woman may have an orgasm quickly, this does not indicate full arousal. If the goal is to have an orgasm, the genitals are wired to get you there. If the goal is deeper intimacy, meaning more intentional heart-centered approach, then having an orgasm is only an aspect of the encounter, but not the goal. When we first encounter a love relationship, that passionate spark makes us feel alive and that we’ve met the one and only (rationalizing all the other one’s that seem to have fit the bill). Our neurobiological system in on full throttle giving us the primal body sensations to have sex. These physical sensations are quite intense and have a sense of urgency to them for after all it’s “the one.” At some point, maybe even the first date, we have sex and then we just don’t seem to stop. But eventually, the pleasure center tops off and the descent begins. The descent begins with seeing the shadow of the other and who they are with their annoyances, idiosyncrasies, personality quirks, immaturity, emotional unavailability, anger, shutting down, etc. As this emerges, sexual encounters begin to wane and lack that initial charge and power. And another power rears up: the power struggles. One wants it more, the other less. It becomes a chore, either to pursue or oppose the pursuit. Lovemaking went from playful fun and excitement with orgasm being the norm, to a bantering about “doing it” or not “doing it.” And commonly, the woman begins to not have interest in her own orgasm and he stops attempting to please. The passion seems to have run dry and lovers soon become roommates, housemates, and business partners of their household. The question becomes how might we come together to shift these dynamics to re-ignite the passion and create sustainable passion. It is suggested in wisdom traditions through transformation (hence, inner work to do!) of passionlessness, we step into the arms of a sustainable passion. Cultivating a passion that can withstand the ups and downs of the myriad aspects of modernity, requires a process that we each commit to by arousing our heart-centered compassionate nature. The genital-centricity with which is often the primary focus in romantic relationships burns us out. A heart-centered awareness brings the sexual energy up, allowing for connection of the minds. The genitals are quiet proficient at their function so put your focus in a higher realm. To begin, consider not treating your sex life like a McDonald’s drive thru. Begin to slow down the process. If your average time with a sexual encounter is 15 minutes, double the time and don’t rush the process. Engage all the senses, but keep it simple. Turn off all the distractions, phones, computers, TV, chores, etc., and turn toward each other as if that person really matters to you. As Nelson Mandela says, “there is no passion to be found playing small.” When we rush through the most intimate human connection available in our lives, we play small, which suggests that love hasn’t fully emerged. When we take our time and take our sexual encounters slowly, we will begin to notice all the nuances being offered in each moment. As we allow the sensations to be felt slowly and not rushing or forcing it’s intensity, our minds come to the process. When the mind finally settles in this sweet space, love shows itself. So slow down, pay attention as if it your life depends upon it. |
Sherri AikinSherri Aikin is a Fellow of Integrative Medicine, Nurse Practitioner, Sex Counselor, Mindfulness Facilitator, and Life Coach. Categories
All
|
 RSS Feed
RSS Feed